INVASIVE BOWEN’S CARCINOMA OF CHEEK

HISTORY
79 year old woman presented with a 3 month history of right angle of jaw mass hardening over time. A biopsy of a separate lesion of the right central cheek on 2/21/17 showed papillated Bowen’s Disease. The jaw mass was biopsied on 2/24/17 and revealed invasive Bowen’s carcinoma – squamous cell carcinoma.

DISCUSSION
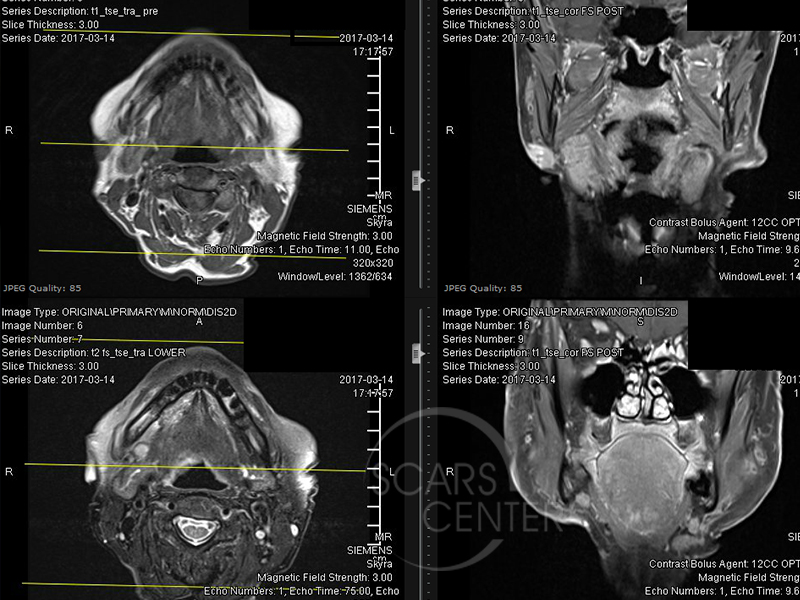
This 79-year-old woman presented with a possibly metastatic Bowen’s carcinoma of the cheek. There were three clinical issues in this patient, which may or may not be related. The obvious one is three-month history of dermal cutaneous mass just below the right angle of the jaw. This was biopsied as papillated Bowen’s carcinoma. Another lesion was a right central cheek papillated Bowen’s disease that was shave excised and cauterized. The workup with an MRI found a 1 cm atypical lymph node in the right submandibular triangle of the neck. The lymph node finding is worrisome as it could represent metastasis from the right angle of jaw dermal nodule. Of course, it could also be unrelated. The discussion at the conference found that both the right cheek lesion and the right angle of jaw nodule both represented papillated Bowen’s carcinoma. The papillated description is of the involvement of the dermal-epidermal junction above the base of the membrane. As the disease spreads, it forms papillae extending into the dermis without penetrating the base of the membrane. The significance of this finding is certain angulation of a histologic section may cut through the papillae without showing its connection to the epidermis. In these cases, a false determination of invasion could be made. However, in this particular patient dermatopathologists expressed confidence that this indeed is a noninvasive Bowen’s disease in the right cheek and invasive Bowen’s carcinoma of the right angle of jaw. The recommendation was to evaluate the right submandibular lymph node with direct excision or sentinel lymph node biopsy. Both cheek and angle of jaw lesions should be excised completely. However, it was predominantly believed that the cheek lesion is unlikely the source of the dermal nodule in the angle of the jaw. The patient has had multiple skin lesions and treatments over the years.
