Recurrent SCC of Nasal Tip
HISTORY
71-year-old man presents with recurrence of SCC of nose following Mohs excision on 2-9-17. Partial rhinectomy was performed with incomplete Mohs excision leaving residual positive margins due to patient’s comfort. Two additional excisions of involved margins were done under anesthesia achieving clear margins. First stage reconstruction was performed on 4-11-18.

Original resection of SCC of the nasal tip and reconstruction. Recurrence presented one year later in the deep tissues of the lateral nasal wall.
DISCUSSION
Management of a recurrent SCC of the nose is challenging. This case represents a 2-phase approach we favor at the SCARS Center for complex skin carcinomas. The first phase involves biopsy mapping of carcinomas to predict the nature of resection and reconstruction required. The second is the treatment phase with Mohs-guided wide local resection.
The patient presented with a recurrent SCC of the nose 1 year after his original SCC treatment with Mohs surgery. The tumor has recurred in the deep subcutaneous space. Multiple mapping biopsies, including intranasal biopsies, have defined where the tumor was not – paving the way for predictive surgical planning.
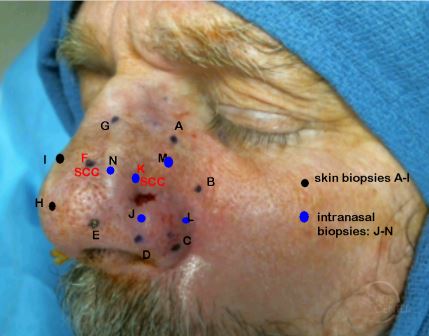
Mapping punch biopsies – 2 mm punch used.
Mohs surgery was then taken to its technical limit. The limit is defined by patient comfort, surgeon technical expertise, and time. The Mohs surgeon inks the remaining positive margin, guiding the surgical resection.
The SCC of this patient was particularly aggressive, spreading through the deep tissues, sparing the overlying skin and underlying mucosa. This behavior was not identified with even deep 2 mm punch biopsies of the skin and the mucosa. Thus mapping underestimated the spread of the SCC.
Additional surgical resection under anesthesia was performed in two more stages to achieve margin control.
The recurrent and deeply infiltrative nature of this squamous cell carcinoma requires postoperative radiation therapy to minimize risk of recurrence.

Defect following Mohs excision of recurrence. Blue ink marks the deep involvement of the SCC in the nasal dorsum.
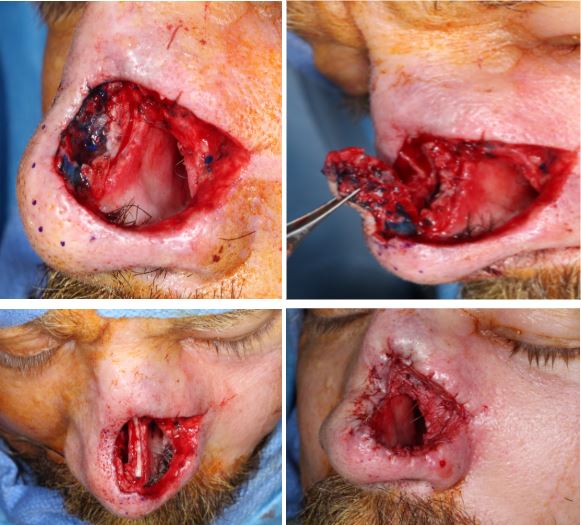
First surgical resection of additional margins under anesthesia.
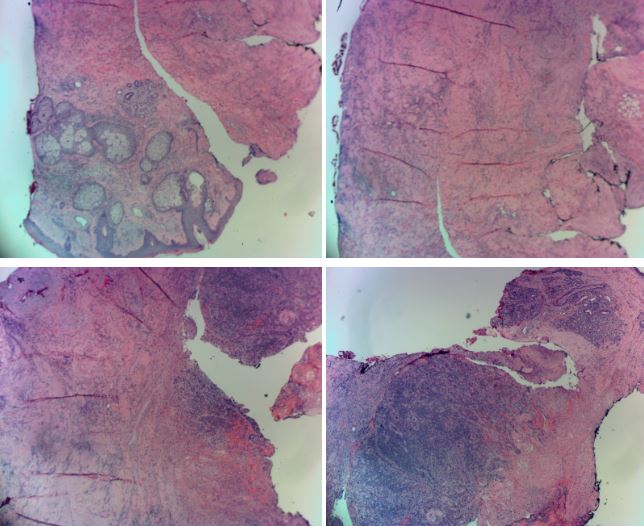
Deeply infiltrating squamous cell carcinoma within muscle and connective tissue. Involved margins in the deep nasal dorsum were still present after the first conservative surgical resection.

Second surgical resection of additional margin. The SCC was spreading within the muscle layer. A strip of skin was taken with the specimen for orientation. Red and blue ink was used for intraoperative marking for histologic orientation.