SCC of Scalp
HISTORY
86-year-old man presents with 3-month history of a mass in the left occipital scalp. 1 year prior, the patient underwent Mohs excision of a large scalp SCC. FNA biopsy on 1-22-18 found atypical squamous cells. CT PET scan showed cancer limited to the mass itself with no lymph node enhancement. Patient experienced progressively increasing tumor pain over the 2 weeks of the work-up. Wide local resection on 3-1-18 achieved clear margins and found no lymph node involvement. Perineural involvement was found in nerves greater than 0.1 mm diameter.

Squamous cell carcinoma metastasis to occipital lymph node 1 year after Mohs excision of scalp vertex SCC.
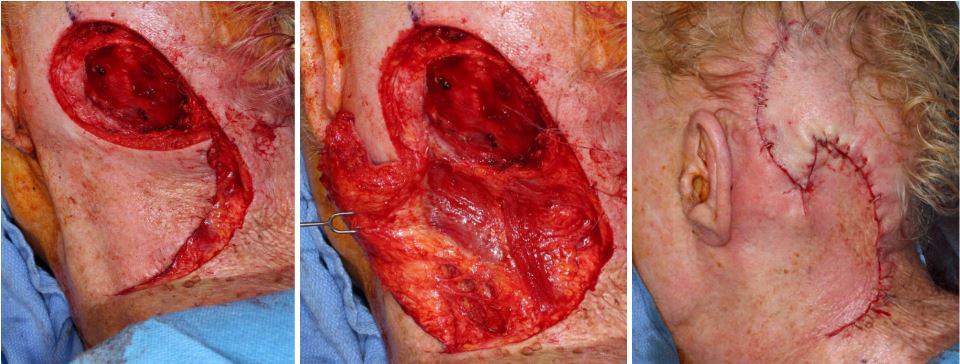
Reconstruction with large scalp and neck rotation flaps.
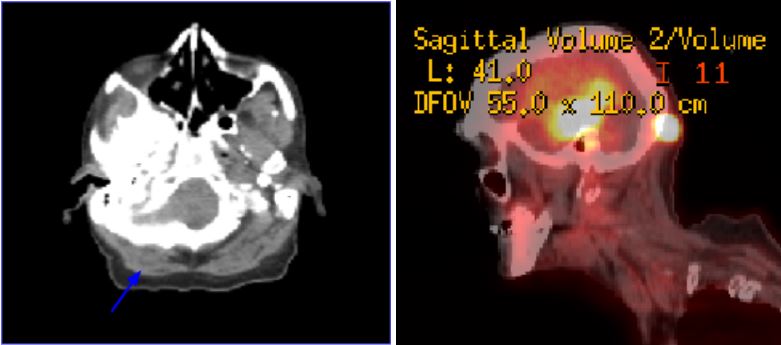
Right occipital scalp mass. CT/PET scan enhancement of the occipital scalp mass.
DISCUSSION
One of the lessons of this case is the need for risk assessment of squamous cell carcinomas of the skin. This assessment need to be done at the time of primary surgical treatment. In this case, the initial scalp vertex tumor was reportedly deeply invading. Deep invasion is one of the risks of metastatic behavior of a SCC. Repeated published studies have demonstrated that the risk of metastases is demonstrable with invasion of greater than 2 mm. Significant risk of invasion begins with 5 mm depth of invasion. Review of literature shows that 2-5 mm of invasion carries a 3-7% risk of lymph node metastases. 5 mm or greater invasion by SCC carries a 14-45% risk of metastases. Recurrence rates are also associated with depth of invasion: 2-5 mm recur 3% of the time and 5 mm or greater recur 12% of the time in one study. Another related variable is invasion beyond subcutaneous tissues. This is particularly relevant in the lower lip where thinner invading SCC can be already within the muscle. The conclusion from this data points to the need for evaluation and possible treatment of draining lymphatics in some cases. SCC invasion of 5mm or greater deserves consideration of post-operative radiation therapy or lymphadenectomy. In some cases, wider surgical margins beyond narrow Mohs margins are indicated.
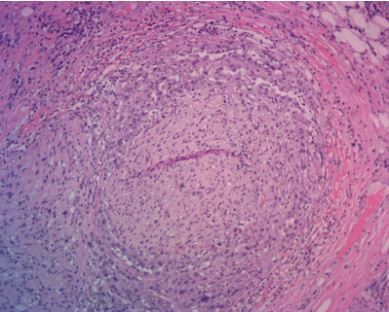
Perineural invasion by squamous cell carcinoma.

