DEEP NECK BASAL CELL CARCINOMA RECURRENCE – FOLLOW UP
Initial resection sparing facial nerve branches

Resection of additional positive margins (the submandibular gland and the mandible are visible),  second excision of additional margin.
second excision of additional margin.
HISTORY
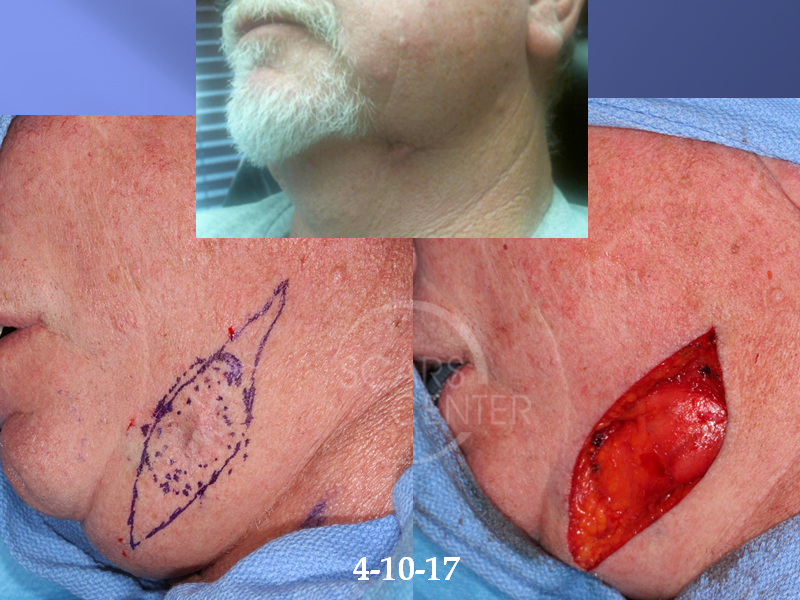
63 year old man presented with a 5-year history of a lesion in the left anterior neck. The lesion was diagnosed as basal cell carcinoma and excised in 2012, but it recurred three years ago with progressive deep scar growth. The lesion was re-biopsied in 2017 as a metatypical basal cell carcinoma with signet ring cell component associated with the old scar. Wide local resection was performed on 4/10/2017. Due to residual deep positive margins, additional deep margin resection, facial lymph node biopsies, and reconstruction was performed on 4/17/2017.
DISCUSSION
The discussion at the conference was centered around the two approaches to this deep neck basal cell carcinoma recurrence. One approach undertaken in this particular case was wide local resection with permanent histology margins. The other would involve Mohs excision. In this particular case, the patient underwent wide local resection with maximal depth of excision, sparing the marginal mandibular nerve branches of the facial nerve. Unfortunately, the margins were positive in the deep margin only. This is the area overlying the fascia over the facial nerve branches. Subsequently, the second stage of resection involved excision of additional margins including facial nerve branches in the fascia overlying the submandibular gland. Resection margin extended to the bone of the mandible and the masseter muscle as can be seen in the photographs. This tissue was sent again for permanent histology with finding of no residual carcinoma.