Reconstructive Cases – Bilevel Grafts
Bilevel grafting with septal cartilage graft and a skin graft.

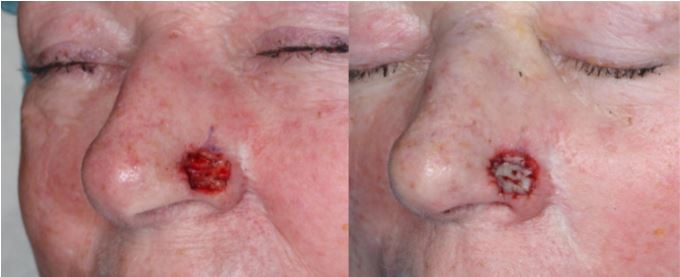
Bilevel grafting 8 days post-op.

Bilevel grafting of nasal ala with an ear cartilage graft and a skin graft. Nasolabial fold partial island rotation flap was used for the cheek portion of the defect.

Bilevel grafting of nasal ala defect.
DISCUSSION
Nasal ala skin defects can be reconstructed with skin grafts generally with excellent results. However, deeper defects of the nasal ala repaired with a skin graft may result in a depressed deformity. Contraction of skin graft healing may also cause retraction of the nasal ala, especially with deeper defects. Adding a cartilage graft to the reconstruction adds thickness to the ala. It also adds structural resistance to contraction.
Because both the skin graft and the cartilage graft requires blood supply for survival, bilevel placement of grafts is required. The cartilage graft is placed under the muscle layer, just superficial to the vestibular skin. The skin graft is placed superficially. Dissection under the muscle layer of nasal ala needs to be limited to 3 mm cephalic to the alar rim. The area close to the alar rim is too thin for dissection and will result in vestibular skin perforation. The sandwich of grafts is secured with full thickness 5-0 chromic sutures. Sufficient thickness of muscle is required to support blood supply after elevation off of vestibular skin.