Deeply Invasive Squamous Cell Carcinoma of Cheek


HISTORY:
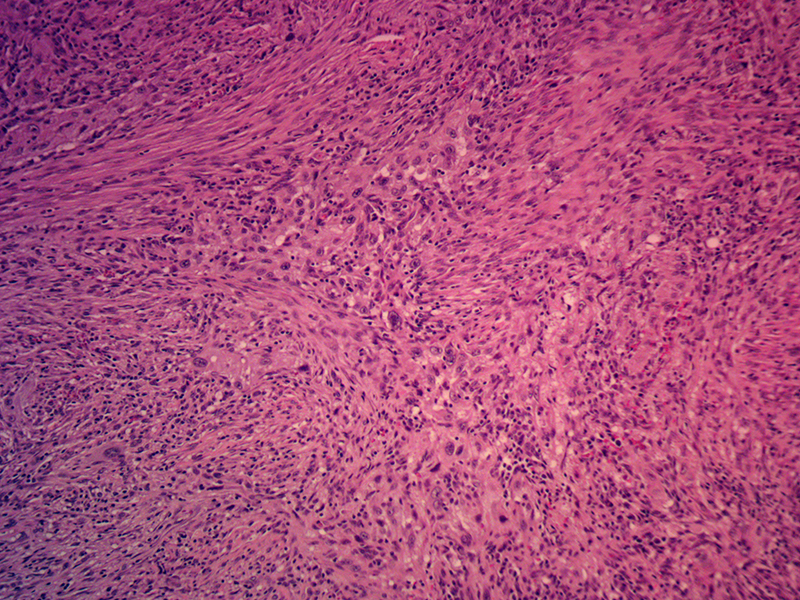
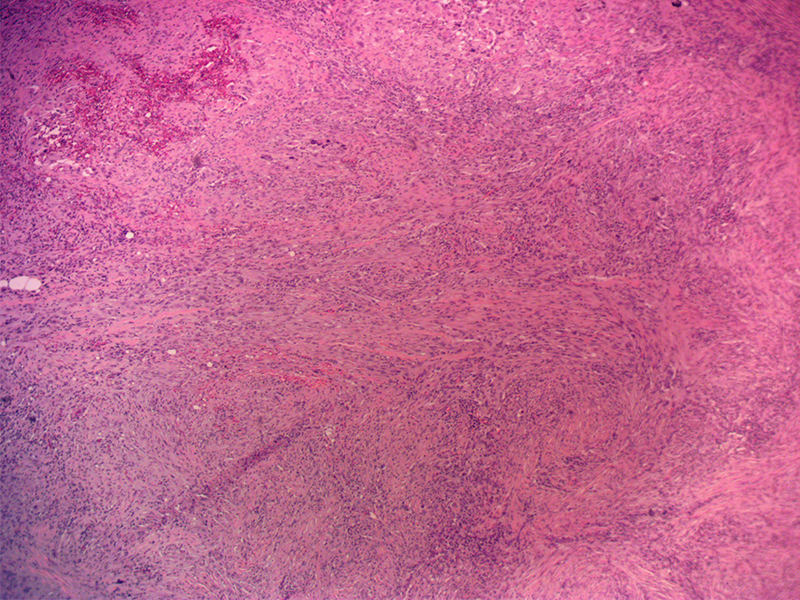
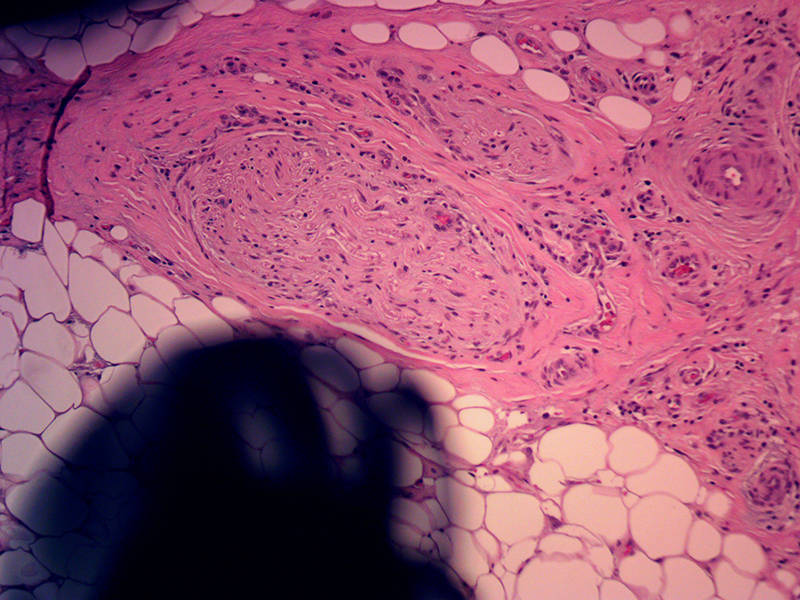
82-year-old man with a 1 year history of squamous cell carcinoma on the right lower cheek biopsied on 4/28/2017. Radical resection of the right cheek carcinoma and deep facial lymph node biopsy was performed. Intraoperative Mohs margin evaluation confirmed clear margins. Final permanent histology margins were close but clear. Evidence of perineural invasion was present.
DISCUSSION:
This deeply invasive carcinoma represents a high-risk lesion. The depth of invasion is greater than 1.5cm. Although margins were clear, they are close by oncologic standards. The lowest margin of clearance in the surgery was approximately 5 mm. High-risk squamous cell carcinomas can metastasize to regional lymph nodes and to distant sites. Local intradermal metastases or even skip lesions are possible with a high-risk carcinoma. The treatment of high-risk carcinoma requires additional radiation therapy to the local site of tumor as well as to the regional lymphatics in case of lymph node metastasis.
Further workup of this patient requires a CT/PET scan to check for regional and possibly distant metastases. There are several factors that support conservative management – observation for recurrence. The first finding for conservative management is the negative lymph node in the draining lymph node chain of facial lymph nodes. Second factor is that the squamous cell carcinoma has been present for over six months with no clinically obvious cervical lymphadenopathy. Finally, the advanced age and poor medical state of this patient supports less aggressive management. Even local radiation to the cheek can be disabling with oral mucositis. Regional radiation to the lymph nodes of the neck would cause significant disability with this patient, perhaps even requiring G-tube placement for nutritional supplementation.
Ultimately, the patient needs to be intimately involved in the decision making with all these factors presented to him for consideration.
The resection of this patient’s SCC involved facial nerve branches resulting in paralysis of perioral muscles. At the time of reconstruction the patient was treated with a static lip lift and corner of mouth elevation.
