MAPPING OF BCC WITH CONFOCAL MICROSCOPY






HISTORY
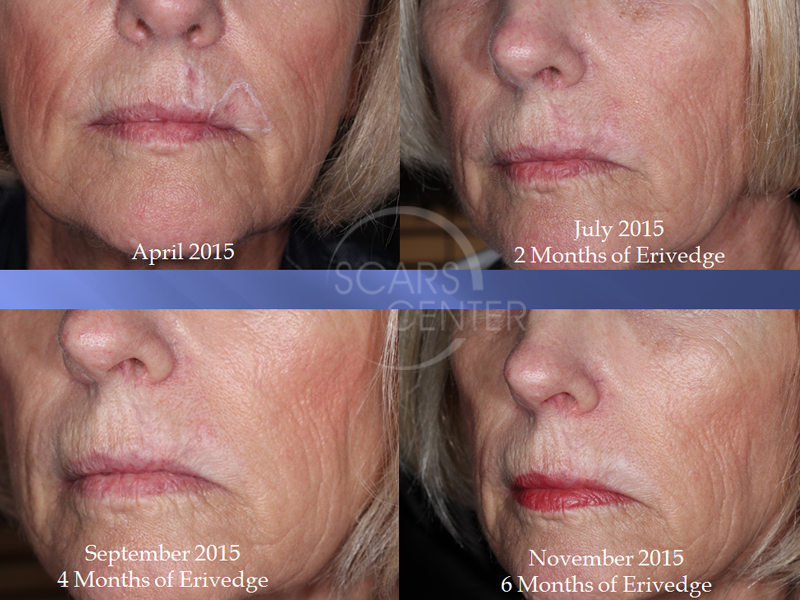
63 year old woman diagnosed with recurrence of BCC of left upper lip in 2015 after treatment of Efudex and a surgical excision in 2005. Patient had 3 separate BCC locations in left upper lip. Due to the size and multifocality of the lesion, patient was treated with Erivedge for 7 months with a partial response. Residual BCC was treated with Aldara (imiquimod) for 5 weeks and a couple of cycles of PDT (photodynamic therapy). A residual left upper lip BCC was then mapped with confocal microscopy and treated with Mohs excision.
DISCUSSION
This patient presented for her recurrent or persistent basal cell carcinoma after a long history and struggle with basal cell carcinoma of her left upper lip. Initially, the patient was diagnosed over a 1 1/2 years ago with multicentric basal cell carcinoma of the upper lip. Both surgery and radiation therapy were declined by the patient and instead, she underwent seven months of treatments with Erivedge. Erivedge was not completely successful as the patient subsequently required additional treatments with Aldara and photodynamic therapy to try to clear this superficially residual basal cell carcinoma. Finally, the patient had one clinically obvious lesion of basal cell carcinoma, which we treated surgically.
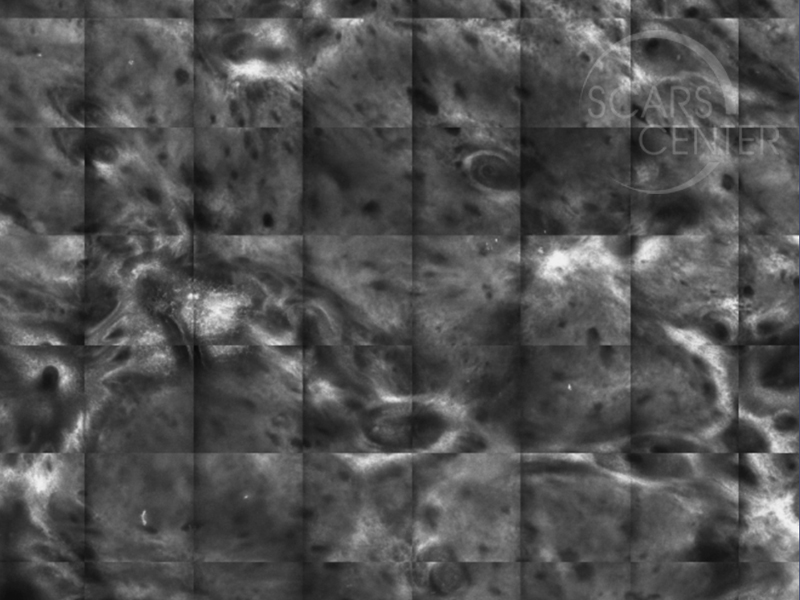
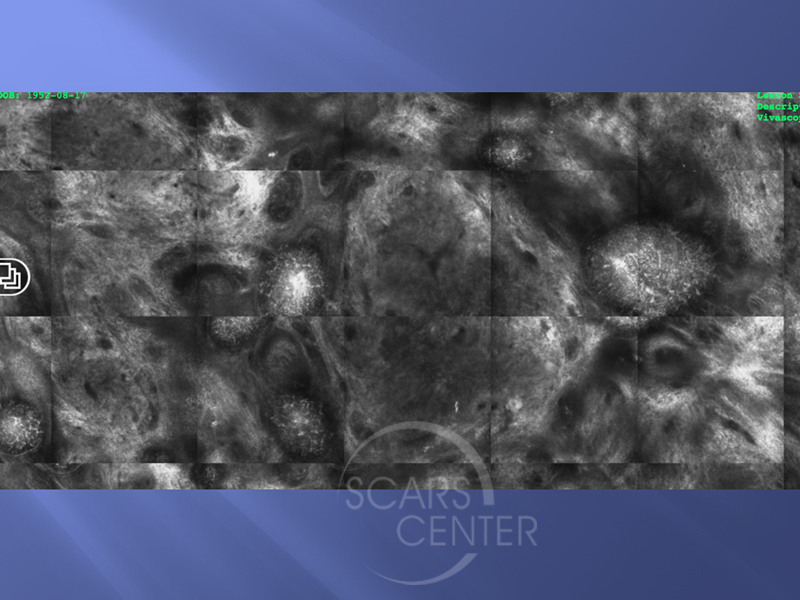
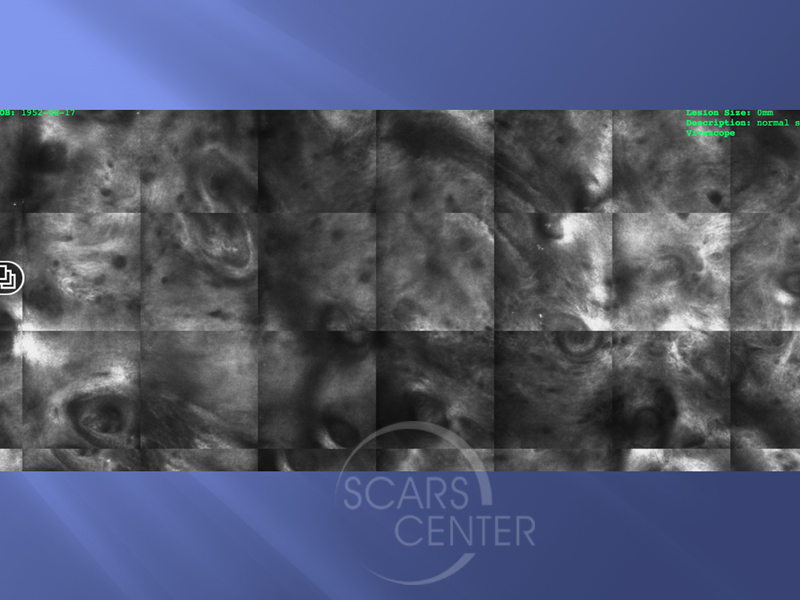
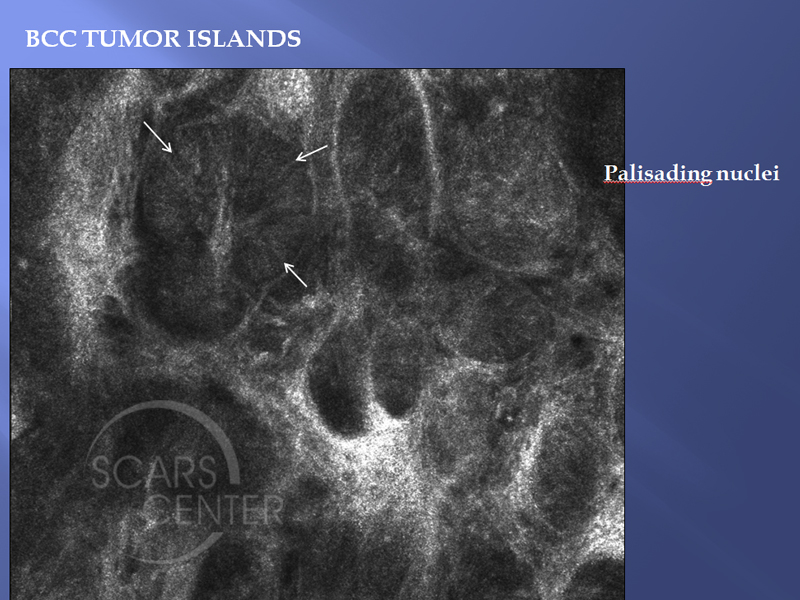
What is interesting about this patient is how we planned her treatment. Again preoperative planning and mapping of cancers is very helpful for the reconstructive surgeon and also for the patient. Instead of mapping surgical biopsies, we have chosen to use reflectance confocal microscopy to evaluate the extent of this carcinoma. The photo illustrates locations of reflectance confocal microscopy imaging. The imaging area is about 8 mm in diameter. It is not a quick process, as each spot requires about 20 minutes to image. The evaluation of the images is currently done offsite via the internet by experts in reflectance confocal microscopy. Locally, Dr. Michelle Aszterbaum, a local dermatologist and an expert in RCM, validates the findings and correlates with the clinical scenario. Once it was determined that the basal cell carcinoma was localized in a small area of the upper lip, then Mohs was undertaken. The Mohs surgery and reconstruction were quite predictable for the patient and for the surgeons.
This case represents that tumor mapping could be done with a noninvasive modality – reflectance confocal microscopy. Its limitations are that it requires 20 minutes to acquire an 8mm image and that it can only image a flat area. The procedure can be performed by a medical assistant once the physician has planned the imaging. Image interpretation still requires a validation by a remote expert via the internet.