BASOSQUAMOUS CELL CARCINOMA INVADING DEEP PAROTID
HISTORY
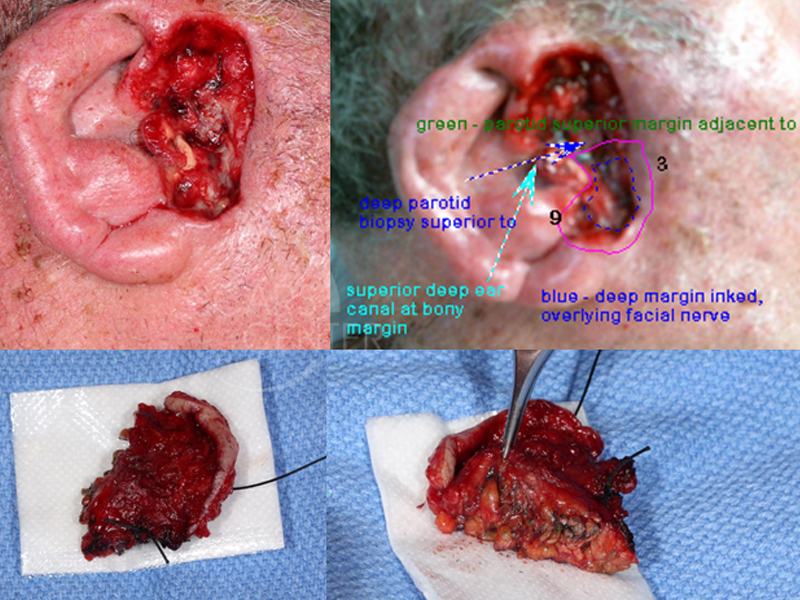
79 year old man presented in 3/2017 with basal cell carcinoma of the left tragus, involving the parotid and the tragal cartilage. 3 levels of Mohs were done with positive deep margins. Mapping biopsies were performed on 3/20/17.
DISCUSSION
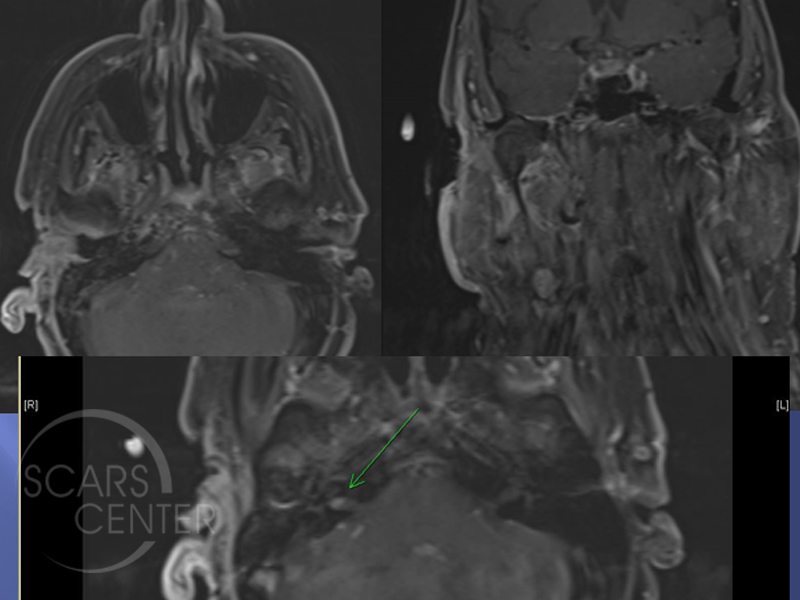
This is the case of 79-year-old man, who presented with deeply invasive basosquamous cell carcinoma of the right cheek and the parotid gland. Mohs excision after three levels was able to clear cutaneous margins, but found the tumor invading deeply into the parotid gland. The patient presents for evaluation and additional treatment of this deeply invasive basosquamous cell carcinoma. The patient has been evaluated with an MRI, which showed no invasion into the infratemporal fossa. However, facial nerve involvement could not be ruled out. As a result prior to undergoing definitive resection, the patient underwent staging biopsies. This included facial nerve dissection to determine the extent of the nerve’s involvement. Final pathology revealed the main trunk and both major divisions of the facial nerve free of both gross tumor and histologically involved tumor. The deeply invasive tumor was still present cephalad to the facial nerve and was not resected pending completion of workup and surgical planning. The tumor grossly involved the temporal branch of the facial nerve.
This case represents the complexity of carcinomas invading the parotid gland. Main modality of treatment is either surgical or with radiation on these cases. However, if the tumor grossly involves the facial nerve, then the necessary treatment would require facial nerve resection in order to achieve the surgical cure. With basal cell carcinomas, this may not be an acceptable scenario. Facial nerve resection is severely functionally impairing and emotionally upsetting. Therefore, preoperative treatment planning is critical in these patients.
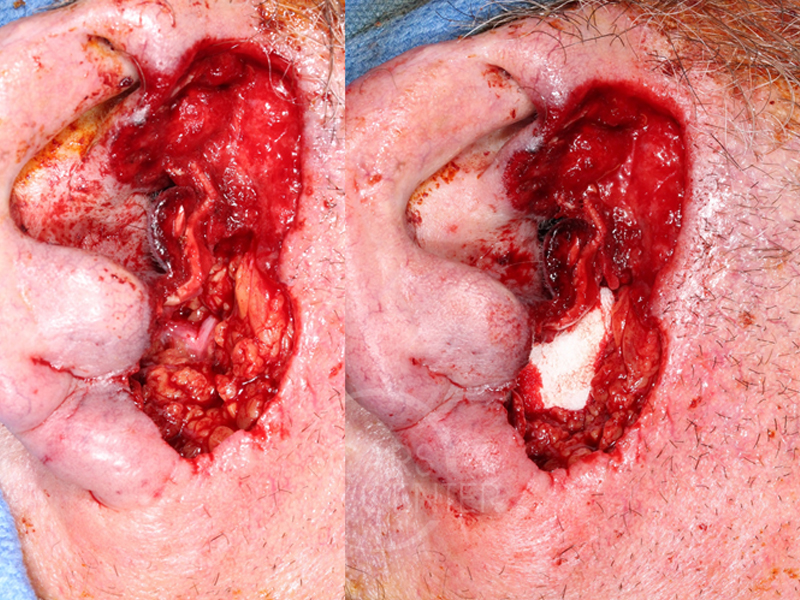
This patient is unusual in that we have chosen to perform a facial nerve dissection in order to define its invasion prior to definitive treatment. This helps prepare the patient for the comprehensive surgery and to prepare the surgeon for the possible reconstruction required. Although, the main trunk and the two main divisions of the facial nerve were found to be free of cancer, gross involvement of the tumor was in the area of the temporal branch of the facial nerve. As a result, the patient was prepared for resection of that branch. This is not an essential nerve and would only impact the movement of the forehead on that side. The wound was not closed, but the facial nerve area was packed with Gelfoam to separate the gross tumor above that from the exposed facial nerve below. This patient will require a definitive resection of the temporal branch of the facial nerve and a portion of the external auditory canal. The deep margin resection will likely be deep temporalis muscle fascia near the zygomatic arch. The superficial temporal artery will likely be scarified with this resection. Postoperative management of this patient will require radiation therapy to the region. If lymph node involvement within the parotid gland is discovered, then additional radiation treatment of the upper neck lymphatic chain would be required.