Mitoses in a Dysplastic Nevus
HISTORY
61-year-old man presents with 6-month history of forehead lesion. Biopsy on October 2017 showed atypical nevomelanocytic neoplasm with several mitoses (3/mm2). An excision with 5 mm margins was performed in November 2017 with negative findings.

Dysplastic nevus with mitoses.

Excision of forehead lesion with temporary closure using a porcine xenograft.
DISCUSSION
This melanocytic tumor of uncertain malignant potential can also be called a MELTUMP. These lesions present a treatment dilemma. Wide excision with at least a 5 mm margin is necessary. More aggressive approach with sentinel lymph node biopsies can be considered. In this case, given the small size of the lesion, a less aggressive approach was undertaken. The determination should be made by a surgical melanoma specialist. Consideration of risk of sentinel lymph node biopsy needs to be made.

Reconstruction with TPF island flap.
From a pathologist’s perspective a simple adage is descriptive of the issue. “You cannot be proven wrong if you call all melanocytic lesions melanomas.” Clearly, it is not in the pathologist’s interest to err on the side of a more conservative approach. But it is a surgical specialist’s responsibility to weight the risks of more aggressive surgery versus the risks of a more conservative approach.
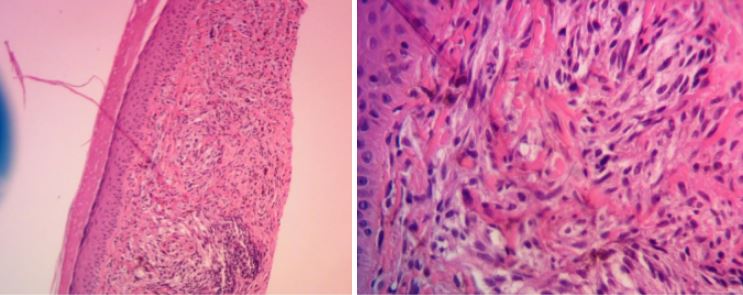
Atypical nevomelanocytic neoplasm biopsy. The microscopic differential diagnosis would include a severely atypical compound nevus or severely atypical cellular blue nevus. Note mitotic figure on the high power photomicrograph.