Management of Recurrent Large Melanoma In Situ
HISTORY
78-year-old man presents with a recurrent melanoma in situ of left cheek in April 2018. Previously, the melanoma in situ was excised in 2001. Patient’s dermatologists performed excision in three stages over a period of 3 weeks to achieve clear margins. Reconstruction of left cheek was performed with a cheek and neck platysma myocutaneous island flap.

Fig. 1. Final defect after three serial excisions of the cheek melanoma in situ. Defect size is 6.5 x 6 cm.
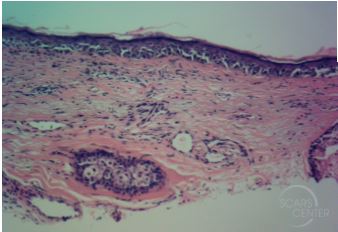
Fig. 2. Melanoma in situ histopathology.
DISCUSSION
Melanoma in situ in extensively sun-damaged skin can present with clinically indistinct lesion. Predicting margins can be difficult as was the case here. There are four approaches to treatment of such large lesions.
- Serial excisions with permanent histology margin evaluation can be done as in this case. With a good dermatopathology laboratory, serial excisions can occur every 48 hours, the minimum time necessary for lab processing and slide reading. In some cases immunohistochemistry staining (SOX10 or MART-1) is required which may prolong result reporting to 3 days. SCARS Center uses Laguna Pathology Medical Group that is able to achieve this turnaround time.
- Anticipated margin excision with primary closure of the periphery leaves the central tumor specimen intact. This involves excising the outer margin of the tumor with permanent histology evaluation and closing the wound. (Fig. 3) With no open wound left, the time pressure to diagnosis is removed. Once clear margins are achieved, the central specimen can be excised. The risk is surprise diagnosis of invasive melanoma within the central specimen. See the article presenting such scenario. (Fig. 4)
- Mohs excision of margins of a melanoma in situ. Majority of the the central specimen must already be removed and histologically analyzed for evidence of an invasive melanoma. Special experience is required for reading of melanoma in situ Mohs slides.
- Mapping biopsies prior to resection is a useful approach that avoids leaving the patient with an open wound while waiting for pathology results. 2mm punch biopsies are usually the method employed at SCARS Center. See the article discussing this in greater depth. This approach does not address a comprehensive central specimen evaluation and must be paired with an approach addressing possible invasion within the central specimen.

Fig. 3. Anticipated margin excision of the leg melanoma in situ.